Learn how our community's safety is impacted. Sex offense civil commitments currently create a human rights crisis and wastes taxpayer money. Join The Journal of Ethical Resource Allocation in Mental Health in advocating for change through known evidence-based insights and innovative strategies for progress.
Isn't it alarming that a human rights crisis misuses taxpayer money?

Cost of Care for Unnecessary Services in Civil Commitment Scheme
An Examination Of Fraud, Waste And Abuse Upon Cost Of Care Billing Practices For Mental Health Services Found Not Necessary At Minnesota's Sex Offender Program
Brad Stevens, Chairman Emeritus of the Moose Lake Resident Advisory Family Council (RAFC); Alec Cook, Chairman of the Moose Lake Resident Advisory Family Council (RAFC)
ABSTRACT:
Civil commitment is a restraint on individual liberty that occurs at incredible expense to the State. As a result, good public policy has always been to limit civil confinement only to those individuals who have been found dangerously mentally ill by the courts. In the case of the Minnesota Sex Offender Program (MSOP), the State has an interest to protect the public from sexual violence and rehabilitate the mentally ill. Both the Minnesota and United States Supreme Courts, in regard to the standard of care provided at civil commitment facilities such as MSOP, have established that the State has considerable discretion in determining the nature and scope of its responsibilities in developing treatment regimens. However, both state and federal courts have clearly established that this form of confinement is reserved exclusively for those in need of medical care, concluding that the State serves its purpose of treating rather than punishing sexually dangerous persons by committing them to an institution expressly designed to provide psychiatric care and treatment. Similarly, the Minnesota Supreme Court has held that the Minnesota Commitment and Treatment Act (MCTA)—the law which governs the MSOP civil commitment scheme—protects civilly committed patients' due process rights so long as procedural safeguards that include periodic re-evaluation and competent medical care and treatment are provided. Absent absolute adherence to these strictures, civil commitment devolves from a remedy for those with authentic medical needs for severe mental disorders into preventive detention for those reviled by society. This is exactly what has occurred: MSOP, through their senior management team, knowingly detains patients with no medical needs and then defrauds the taxpayer. The evidence for this is provided below.
Fraud, Waste and Abuse: The MSOP Bills Both the State and Federal Government for Services Not Provided
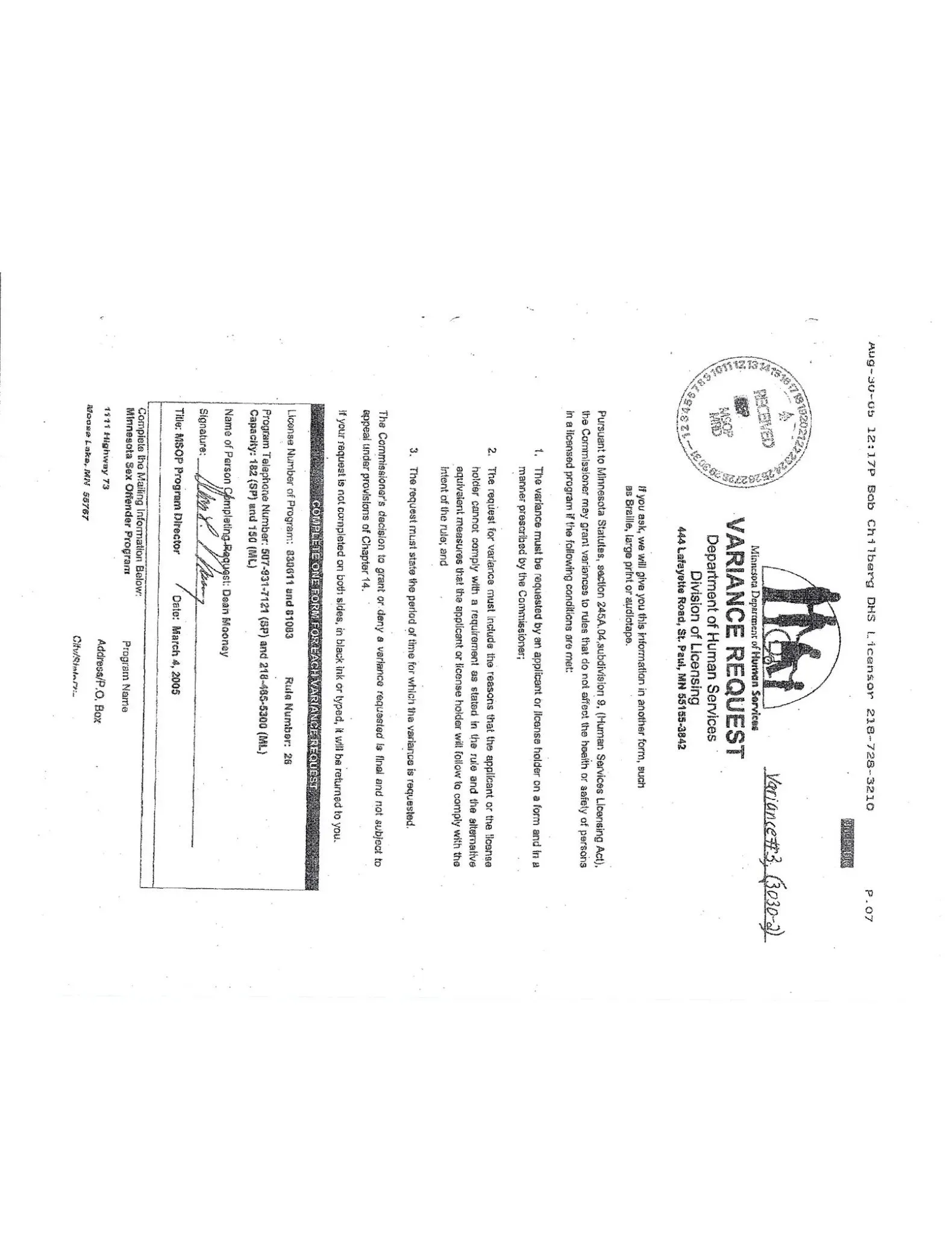
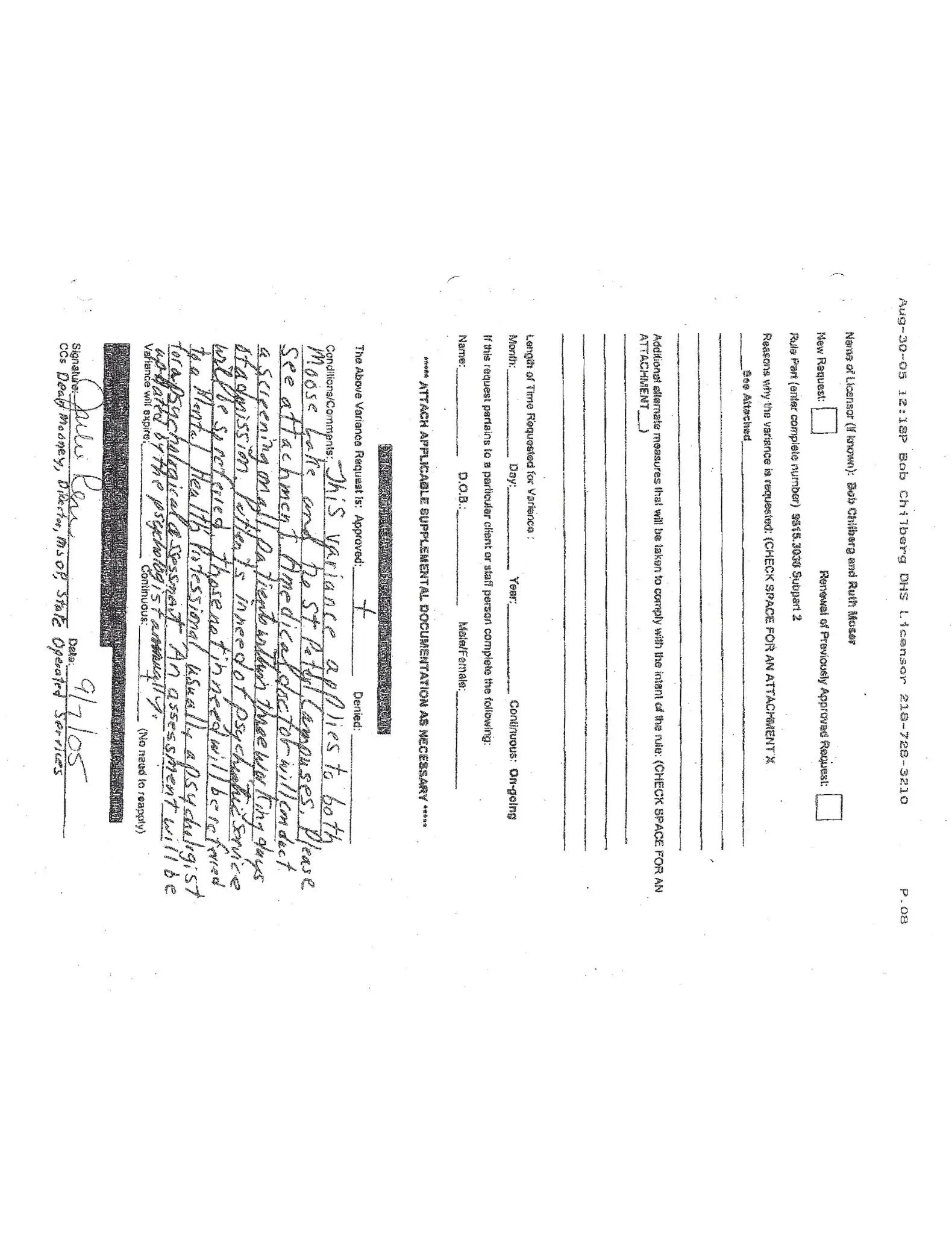
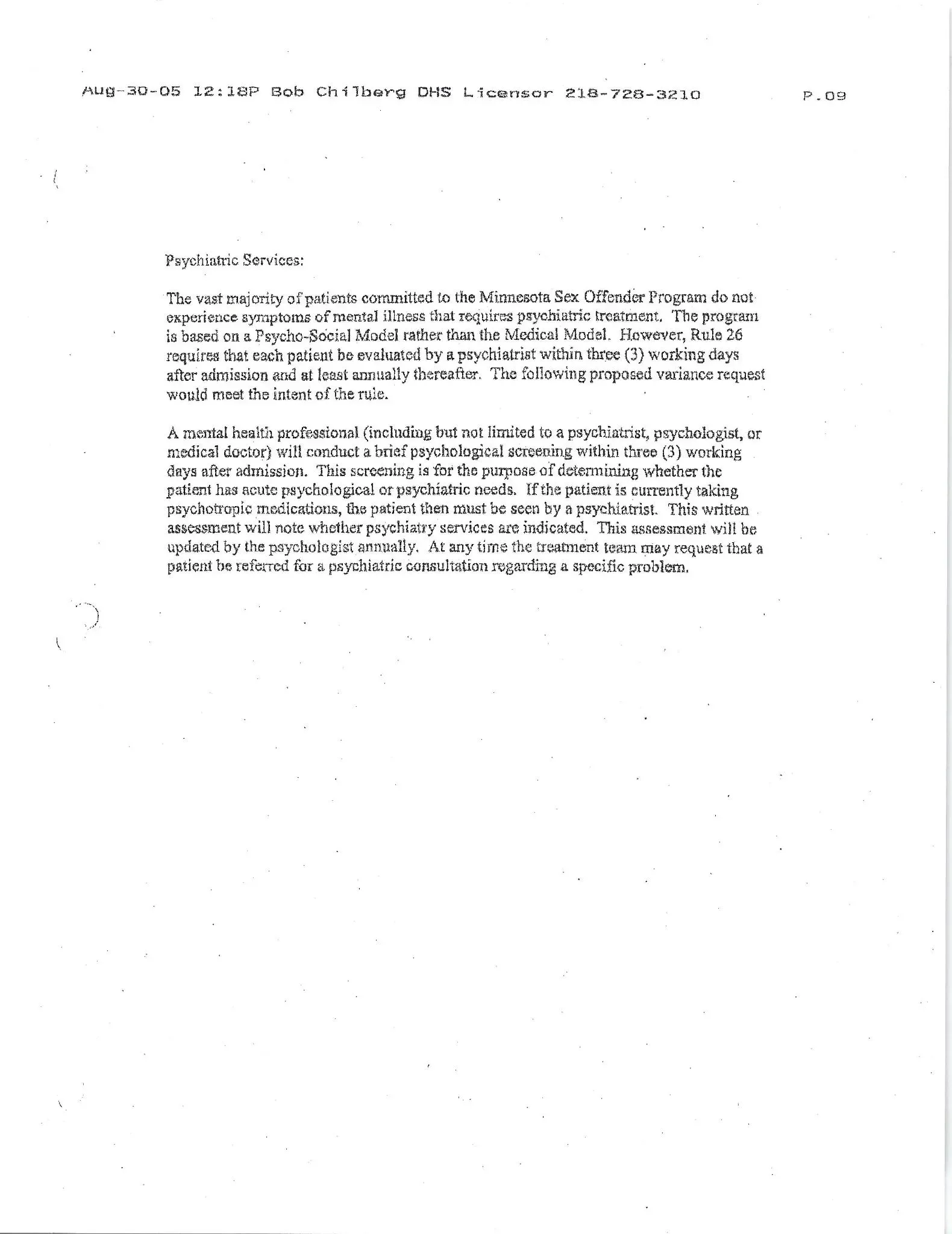
As part of their requirement to follow the laws as set forth by the Courts to protect the due process rights of civil confinees, the MSOP has historically had to follow certain administrative rules. However, in 2005, then MSOP Executive Director Dean Mooney requested a NON-PUBLIC variance from the Department of Human Services (DHS) Licensing Division owing to perceived difficulties of operating the program in accordance with the law. Specifically, the rule to which Mooney requested exception to was Administrative Rule 9515.3030, subpart 12, which states: A psychiatrist must evaluate each person within three working days after the person is admitted and re-evaluate each person at least annually. This rule is consistent with the due process guaranteed to civilly confined patients by the Minnesota Supreme Court. Mooney, in answering the application's requirement for a reason as to why the MSOP could no longer comply with the rule necessitating psychiatric evaluations, stated: The vast majority of patients committed to the Minnesota Sex Offender Program do not experience symptoms of mental illness that require psychiatric treatment. For unknown reasons contrary to judicial precedent, the DHS approved this variance, thus committing fraud and championing its further proliferation. In lieu of these mandated psychiatric evaluations, the MSOP began providing annual mental health assessments provided by non-medical mental health professionals such as social workers and license-eligible psychologists in order to determine whether or not patients should be referred for psychiatric care to begin with. Absent a psychiatric referral, there is no medical justification for a patient's continued loss of liberty, and patients' commitments are favorably terminated. However, instead of working to discharge the patient without medical needs—as would be lawful—the MSOP instead continues to detain these healthy individuals for years on end, typically until their death, while billing the Legislature $174,835 per year per patient for medical services not rendered. This fraud constitutes the vast majority of the $126 million dollars the Legislature funds the MSOP with each year. This fraud has drained billions of dollars of State funds over the years. The inherent flaw in MSOP leadership's intentional decision to remove itself from the medical model which justified its lawful existence has been repeatedly pointed out to these very same government officials, yet no rectifying action has yet taken place. MSOP's senior management team appears to be having too much fun with the endless faucet of scarce public resources which the Legislature has entrusted them with. These ignored warnings of fraud have come from a variety of sources:
In March 2011, the Minnesota Office of the Legislative Auditor found that patients at MSOP remain hospitalized despite no longer meeting the criteria of their original commitment. In 2014 during the litigation process of Karsjens v. Jesson (a lawsuit initiated by detained patients challenging the constitutionality of the MSOP), Minnesota's Federal District Court assembled a panel of experts under Fed. R. Evid 706. At trial in 2015, these experts repeatedly testified that countless patients did not belong at MSOP, either in those patients' cost of care, This fraud costs the taxpayer over $126 million each year. commitment, or could be served in a lesser restrictive (and less expensive) alternative. For instance: Dr. Deb McCulloch, a psychologist employed at Sand Ridge Secure Treatment Center (Wisconsin's sex offense civil commitment program), testified: It is my and our [the other Rule 706 Experts'] belief that there are a number of people at Moose Lake that could certainly be managed and be treated at St. Peter or CPS or even in the community. It was our observation, too, that there is likely people that don't need to be provided with supervision or intervention, legal intervention any longer at all but were still at Moose Lake in Phase I [the very beginning stages of treatment]. Dr. McCulloch further opined that, I do believe there are people both at Moose Lake and at St. Peter that could be served in a less restrictive environment. But I also believe—and there's a good example that was presented in the court and in our report—that there are people that should be discharged completely from commitment. Fellow Rule 706 Expert Dr. Robin Wilson came to the same conclusion in even simpler terms, testifying, There are people at the MSOP who I don't believe belong there. Dr. Michael Miner, another Rule 706 Expert, also concurred in his expert opinion, stating that there are people who are in MSOP who no longer meet the criteria for commitment. Dr. Miner then testified that we [the Rule 706 Experts] could name some of them but I do not believe we could name them all, allowing to the simple fact that they had not reviewed the case of every patient at MSOP.
In 2015, Mitchell Hamline School of Law published A Study Of The Efficacy Of The Sexually Violent Predator Act In Florida. 41 Wm Mitchell L. Rev. 780, 813 (2015). The peer-reviewed literature found there is no evidence that shows that state expenditure on inpatient treatment in a secure civil facility is achieving its intended purpose. Even more importantly, the report further stated, neither inpatient nor outpatient treatment appears to have had much, if any, effect in reducing recidivism when compared to the released detainees (no treatment). The 2015 Mitchell Hamline report further included a section titled: A Lesson for Minnesota: Conditional Release and Treatment Efficacy for Persons Considered to Be Sexually Violent Predators. The literature found, with rates of recidivism] as low as they are, even for untreated offenders, it is unlikely that any intervention can significantly lower rates any further.
In 2024, Mitchell Hamline School of Law's Sex Offense Litigation and Policy Resource Center released a damning report entitled Sex Offense Civil Commitment: Minnesota's Failed MSOP for wasting scarce public resources on an ineffectual program with no discernible impact on the incidence of sexual violence. MSOP leadership attended the June 7, 2024 conference at Mitchell Hamline concerning the report, but were seen to have left early. These problems arise directly from MSOP's intentional decision to disobey the law requiring a connection between the medical rationale for commitment and the patient's continued loss of liberty. Consistently, the science shows that the MSOP's detained patients are not of any danger to the public, and that ongoing expenditure on their non-medical treatment is a waste and abuse of tax dollars. Despite these warnings, MSOP's senior management team, who throughout this period has been headed by Executive Director Nancy Johnston, has taken no corrective action of any form whatsoever. All the while, the vast majority of these patients from 2011... from 2015... from 2024... they all remain unnecessarily detained, a breathing emblem of the ongoing bill sent to the Legislature for services not rendered.
Billions of dollars... for what?
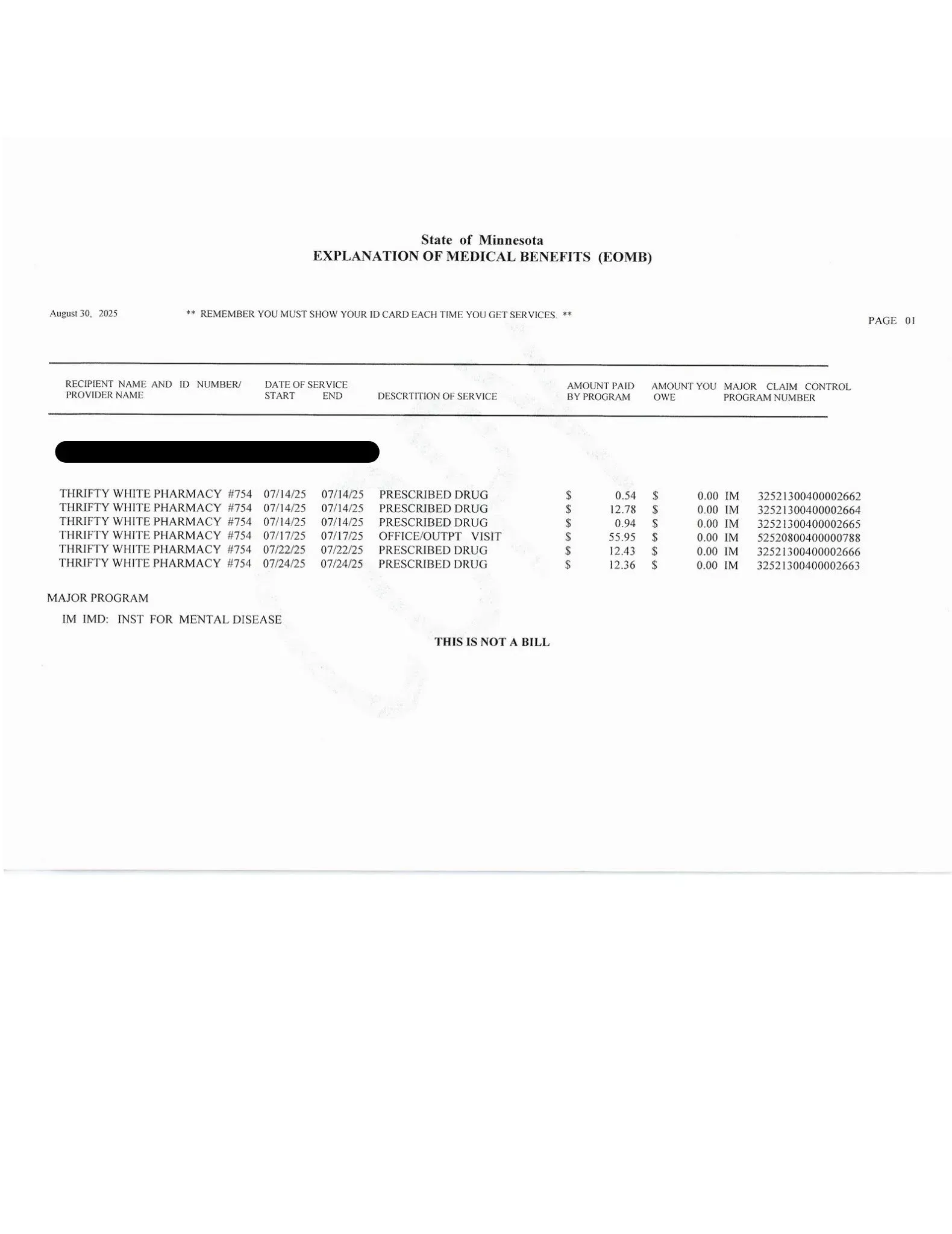
This fraud extends all the way to Washington. Minnesota's counties' Health and Human Services Departments apply for federal grants to be reimbursed for MSOP patients' medical expenses, claiming MSOP to be an institution for mental disease (IMD) as defined by federal statute. However, MSOP does not meet the definition of an IMD. An IMD, as defined by federal law, is a hospital, nursing facility, or other institution of more than 16 beds that is primarily engaged in providing diagnosis. treatment, or care of persons with mental diseases, including medical attention, nursing care and related services. Federal regulations make clear that whether an institution should be considered an IMD is determined by its treatment of individuals with mental diseases, whether or not it is licensed as such and overall character as that of a facility established and maintained primarily for the care and treatment of individuals with mental diseases. The overall character of the MSOP is to provide confinement and non-medical treatment for risk factors, not a diagnosis, contributing words of Nancy Stacken, the clinical director at the MSOP - Moose Lake facility, Dynamic risk factors, not a diagnosis, are what a person can intervene on their risk to reoffend by addressing their dynamic risk factors in treatment. It is the goal of MSOP and... [their] treatment team that patients do not commit additional sex offenses, and targeting dynamic risk factors is the best approach to that end.
Therefore, any reimbursement sought and received by counties for the medical expenses of MSOP patients is fraud upon the federal government. It matters not whether these reimbursements are for physical or mental ailments. In short, MSOP has become the melting pot of rogue bureaucracies defrauding the taxpayer nationwide.
CONCLUSION
The MSOP unlawfully spends over $126 million every year of taxpayer funds upon false pretenses. Civil commitment of sex offenders is explicitly limited to those who require medical care for a mental disorder. MSOP's senior management team has deemed that the vast majority of their detained patients do not meet this criteria. However, instead of facilitating the release of these patients, the MSOP senior management team, as headed by Executive Director Nancy Johnston, has intentionally and systematically removed the medical component from their treatment program rather than the healthy patients from their medical program. The MSOP then bills the State and defrauds the taxpayer for these unnecessary services. This is done with explicit knowledge of wrongdoing.
Further, Minnesota counties fraudulently receive reimbursements from the federal government for MSOP patients' costs of medical care when their confinement does not fit the legal criteria requisite to receive such monies. The fraud, waste, and abuse conducted by MSOP's senior management team has become a matter of national interest.
RECOMMENDED LEGISLATIVE ACTION
1. Investigate the MSOP and the counties for fraud, waste and abuse upon cost of care billed to state and federal governments;
2. Audit MSOP for any misappropriations of funds;
3. Examine solutions to reduce sex offense civil commitments and expressly abolish commitments at the MSOP, unless deemed medically necessary;
4. Mandate the Department of Human Services Licensing Board to rescind all administrative variances currently issued to MSOP Facilities. These variances substantially affect and circumvent state and federal legal requirements intended to protect public policy and integrity in mental health care:
5. Facilitate the reduction of the MSOP population to those who are presently deemed dangerously mentally ill requiring psychiatric care and/or pharmacologic intervention for a sexual disorder;
6. Amend Minn. Stat. 253D.27 to include a subdivision allowing patients to petition the committing court for relief. This would allow patients to transition back to the community on provisional discharges through county level Health and Human Services Departments;
7. Remove the Special Review Boards from the reduction in custody process under Minn. Stat. 253D.27 subd. 3. This review process is redundant and an unnecessary waste of taxpayer dollars;
8. Amend Minn. Stat. 253D.27 to mandate the reduction in custody process for MSOP patients to take no longer than 180 days.
9. Absent the express implementation of these other recommendations, sunset the MSOP.
10. Most importantly, reinvest funds once devoted to the MSOP's fraudulent expenditures to primary prevention programs shown to have a demonstrable effect in reducing the prevalence of sexual violence in the State of Minnesota.
This report is authored by Brad Stevens and Alec Cook. They may be reached at 1111 Highway 73 Moose Lake, MN 55767 or via voicemail at (218)-351-1900 ext. 052728 (Stevens) and (218)-351-1900, ext. 117718 (Cook).
Gallery